


Installation view: Fernand Deligny map drawings with cushions (foreground) and works by Fernando Diniz, Arthur Bispo do Rosário, Gustavo Speridão, and others (background). Lugares do delírio [Places of Delirium], SESC Pompéia, São Paulo. April 10th to July 1st, 2018. Photo: Everton Ballardin.
Subverting Care: Reflections and Actions In Between Art and Health
Tania Rivera
Artists, curators and cultural producers today deal with the difficult task of actualizing and defending the power of resistance and emancipation of art in the face of the omnipresence of the cultural industry – consolidated in the last decades of the twentieth century as a consummate convergence between artistic production and marketing – and professionalization and internationalization of the art market – that turns the artwork into a fetish and a kind of bastion of surplus value, even when it actively seeks to question current economic and social conditions. Since the end of the last century, the transformative relational proposals that marked the 1960s adjusted their focus in order to face geopolitical and social issues, while at the same time attempting to construct relational and societal models at the micropolitical level. In recent years, this pursuit has helped to break open the boundaries of the art field in favor of experiential, social and political experiences, updating the modernist dream of uniting art and life with a political dimension and leading to an important questioning about the conditions of exhibiting and transmission of such actions.
In this very rich and problematic field, which now re-positions the question of what art is and its role in people’s lives, and refuses the pretension of so-called erudite art to delimit a place of exception and privilege, we have recently seen several proposals at the frontier between art and health emerging. The terrain of madness and mental health seems to especially affirm itself in this context, reworking under a new paradigm the historical importance exerted by the encounter of modernist critics and artists with the production of psychiatric patients in occupational therapy workshops. In the early 1920s, the “discovery” of such production in Europe contributed to the defense of the “expressive” value of modern art against the prevailing naturalist academicism. Today, once we denounce the arbitrary isolation of people who have psychotic experiences, it becomes naive – or rather violent and segregating – to make them incarnate the figure of the genius, removed from cultural life; that of the so-called “raw”… or “virgin” artist, (to use the terminology of Jean Dubuffet in the expression art brut and its reworking by the Brazilian critic Mário Pedrosa). What meaning could such a term have in the field of contemporary production where neither technical training nor critical reception guarantee the place of the “authentic artist” nor the “raw”? Although there are still galleries of outsider art worldwide, it may seem problematic today to incentivize the production of “outsiders,” seeking to highlight their work, as this would paradoxically enhance their supposed distinction from “artists” in general. So what then is the purpose of current artistic proposals in the field of mental health? To confine art to the supposed curative goals of “art therapy”? And in the context of artist residence projects or other interventions in mental health institutions? Is it about “caring” for patients?
Caring is power
“Care” seems to me to be a very dangerous word in this context. Under its auspices, terrible acts have been committed, especially in the area of mental health: beginning in the late eighteenth century, hospices were created to remove people from their social and affective context, where they were subjected to the most arbitrary of treatments, disrespectful when not painful, and even mutilating their physical and mental integrity. Moreover, the spaces of segregation thus structured, which remained hegemonic in the treatment of these psychiatric disorders until recently (and is still in use to some degree, it must be admitted), housed not only people with intense psychic suffering, but also served as a depository or prison, in Brazil and in much of the world, for people who acted in ways considered morally wrong by their families or even for political opponents of shady governments.
For this reason, it should not be forgotten that the act of caring always implies a relationship of power, as much in the health arena, between professionals and patients, as in social relations more generally, including the family: between adult and child, father / mother and daughter or son, there are affective, moral, and legal obligations that sometimes seem to hide the political game present there. The ideology of care implies that on the one hand we have A – one in need of care – and on the other B, the one capable of ministering such beneficent actions, supposedly doing this for A. It is important to scrutinize each particular situation in which such a generic structure resides to get to the questions that its simplicity tries to hide, such as: who supposes that A needs care? Does he himself, B who cares for him, or even a third, C, who may or may not be a representative of a particular professional, religious or juridical category? And in case the demand for care comes from others, does A agree or hold the power to refuse them? Is it possible to have situations of reciprocity, in which the care that B directs toward A symmetrically correspond to actions of a similar kind from A to B? And yet, what is the degree of specificity of such actions, given the singularities of A and B and the situation between them? Will there come from position C a demand or requirement of standardization that turns the care or treatment into predetermined actions that barely take into account the particularities of each situation between A and B?
The questions are numerous, and I will limit myself here to lay out a few of them, trying to show the complexity of the political situation of “care,” “treatment,” or even more specifically, “therapy”. In this very vast terrain, I would like to emphasize the psychoanalyst’s position in its particularities. I believe that psychoanalysis, far from willingly submitting to the idea underlying this chain of terms (or, on the contrary, refusing it peremptorily) is rather a practice that defines itself as placing these terms into question, in as far as it is particularly concerned with the relationship between A and B – without losing sight of C – explicitly and centrally, through the concept of transference.1 It seems to me that psychoanalysis is not simply a practice of care, within the field of institutional services, but a critical practice of “care.” Or perhaps we must admit that it does not necessarily lead to critical action, depending on the professional and the situation in which he or she and the analysand are inserted, but such potential is fundamental.
In the field of medicine, the power of the professional over his/her patient has always been an implicit generator of the success of treatment, acknowledged and reinforced by the majority of the medical profession, in a zealous attitude of maintaining privileges that count on the weapon of drugs (in partnership with the pharmaceutical industry) and the protectionist and corporate action of regional and federal councils. Within this general structure, the suggestive virtues of medical discourse are often brought to the forefront, in relation to the patient’s right to obtain detailed information from the professional and to have a voice in the discussion of the therapeutic decisions to be adopted.
While the suggestive force is thus concealed in medical practice under the discourse of science, so that the power of the physician remains unquestioned, in the field of psychoanalysis it is recognized and managed in such a way that the underlying power structure is subverted. This is because, in the first place, the practice of the psychoanalyst rests on listening to the analysand, even if the analyst agrees to assume the place of supposed knowledge that enables him or her to be addressed. Only the “patient” holds the knowledge that is unveiled, and therefore his/her position is active and does not correspond to the place of the one who passively receives “care.” Moreover, and more fundamentally, an analytical process must lead to a revisioning and repositioning of the subject in his relation to this Other that would supposedly suppress his/her truth, implying therefore a turning in the structure of power and a certain liberation from the position of being subjected.
But is such “liberation” restricted to the private scope of the individual practice? I believe that this is a fundamental question for psychoanalysis today, even for psychoanalysts in exclusively private practice. And it is unavoidable for those who work in mental health institutions, whether public or private.
A Brief Testimony Marked by Psychoanalysis
I believe that institutional psychoanalytic practice should seek to set in motion the care (or rather the power) relations that exist there. In order to advance in the attempt to characterize this action, I will refer to one of my own professional experiences, many years ago, in the mid-1990s, at the Foyer de L’Équipe in Brussels, pioneered by the Italian psychoanalyst Alfredo Zenoni. The institution defines itself as a post-crisis or residential therapeutic community that welcomes adults with difficulties for a period of six months to two years to prepare for their return to life outside institutions. The presence of psychoanalysis is fundamental, not as one of the modalities of care practices, but rather as an instrument of “dislocation of the institutional apparatus,” as per Zenoni’s expression. I will not be able to detail here how their everyday mode of functioning enables small dislocations that seem to me to have a much wider “therapeutic” dimension than the mere remission of symptoms.2 I will content myself in mentioning, in a testimonial and personal way, some of my experiences there, which have become the hallmarks of my clinical practice, as well as my intellectual posture, even though a few years afterwards I stopped working directly within mental health institutions.
As I said before, psychoanalysis was not present in this institution through psychoanalytic consultations, although part of its team is made up of psychoanalysts, who work alongside professionals with diverse backgrounds, such as psychiatrists, nurses and socio-therapists, among others. Given the focus of the restructuring of the subject’s life to function outside any institution, he/she was encouraged to seek individual treatment outside the Foyer. Within this practice each patient had a team member as a point of reference for establishing and monitoring their individualized treatment project: choosing among the varied collective activities that marked the daily life of the institution, assuring part of its practical needs (such as mowing the grass, for example), and eventually moving out of its physical jurisdiction.
In this way, the operation of the Foyer did not take place in a centripetal manner and delimited by the exterior, but was rather marked by centrifugal vectors. One of the strategies of the “ventilation” of the institutional environment was the presence of interns like myself, who did not have clear tasks to fulfill and spent many hours in the institution interacting with everyone; being there as-it-were in that context with our desires on which we would draw to propose workshops and activities. After some time adrift, I proposed a movie activity on Friday nights. The activity was very well received and unfolded in a lively way over several weeks: we discussed what movie we wanted to see and then we took the subway to the cinema, together. There were between seven and ten of us, and no one – not ourselves nor other team members, or the “patients” themselves – ever worried about the possibility of any negative occurrence or incident or how I would be able to handle it, particularly in view of my young age and inexperience and my limited knowledge of the city and its mental health network (remember there were no cell phones yet).
Such a situation could be seen by some as one of a lack of “care.” But rather it seems to me to serve as an indication of an ethical stance of respect for the subject that can eventually provide therapeutic and even transformative effects of the subject’s position in the world. Such a stance implied the emptying out of the task of “curing” in favor of prosaic actions in daily life, which accompanied a painful self-critique of my claim (of my power) to “treat” and the acute awareness – and acceptance – of my impotence in the face of the complexity of human pain and beauty that the psychotic experience offers. Moreover, such an ethical posture implied a certain risk, correlated to a gamble: the gamble on the autonomy and capacity of the subject went hand in hand with a very transformative subjective act, which has provided the direction for my path as a psychoanalyst ever since: the act of welcoming the suffering of another without seeking to “protect” him or her, but facing the pain in order to assume (with the body, in his or her own body) the risks and dangers that it carries.
Another brief recollection reinforces the question of danger and how the institution did not seek to illusorily remove it from everyday life: in regular cooking activity, knives were within the reach of the “patients”, and in fact one day one of them used one of them to threaten a colleague.
At the Limits of the Body
This formative experience no doubt resonated, years later, in 2012, when developing an artist residency program at the Heloneida Studart Women’s Hospital, in São João de Meriti, in the region known as Baixada Fluminense. The project was initiated via the invitation of Dr. Ana Teresa Derraik, then clinical director of this maternity hospital – attending high-risk patients – and relied on her attentive follow-up. Such an invitation was part of the goal of “humanizing” hospital care, and it seemed to me to be simply impossible to refuse. In the first place, it was remarkable that the invitation came from the institution itself, thanks to Dr. Ana Teresa’s vision and knowledge of contemporary art, and that the residencies would be inserted in a clinical, managerial and political project to defend women’s rights. In addition, such a maternity hospital was a rarity in the health context in the country, consisting of a service of excellence performed in an extremely poor urban area with serious issues of violence, bribery and religious extremism. In view of this we saw it as an obligation to support the operation of the hospital and try to contribute to it.
In the first stage of the process, which I led alongside the critic and curator Viviane Matesco, there were only three artists – Barbara Boaventura Friaça, Letícia Carvalho and Roberta Barros – who were to be present in the day-to-day life of the Hospital over a few months, exchanging and being in contact with the medical team and the patients and caregivers that give this context its life. We took a calculated risk that the artists’ unusual presence could contribute to the unpredictable and micropolitical activation of fundamental questions about body, gender and sexuality, power relations in health and beyond, contraceptive policies, religion, etc.
The artists conducted their adventure in the institution in diverse ways, in accordance with their desires and the relational dynamics that they established with the medical team and patients. The process would materialize at some point as a performance or installation in the maternity hospital, but what was in the foreground were our frequent meetings – artists, curators and clinical director – to discuss what went on in the day-to-day lives of the artists in the hospital and outside of it, in life and the social, political and religious context in which this experience took place, which seemed to us at the time to be a kind of cauldron in which many vectors of Brazilian reality were made explicit and especially embodied, with pain and beauty, particularly the questions of gender that we ourselves, as five women, live and have lived, also in the flesh. Assuming that it was a matter of care, the question must be asked in this case: who were we caring for?
I believe that the basic assumption of our actions was that it was not about patient care. We were not there to “humanize” the environment by taking art and “sensitivity”, “beauty” or fun to a hospital. We did not see ourselves as agents of some beneficial action for a needy public. We were involved as subjects with our stories (which included, for some of us, violence and inappropriate obstetric treatment), which does not mean that we underestimated the socioeconomic differences between us and the average patient the hospital treated, but rather that the sociopolitical scope in which the project was inserted was large and complex, and within that we had to recognize our singular positions. We saw ourselves as agents, yes, agents outside the daily life of that institution. That, with our bodies and presence, we could perhaps move or call into question some normalized power relations (especially those between the different members of the medical team and support staff) and a number of “dehumanizing” procedures. Our hope was that the micropolitical situations experienced by the artists and other social actors present could radiate out to some extent, in an unpredictable way.
I cannot do this experience justice here and show how, at the conclusion of the residency, the performance discourse of two of the artists at a medical congress about women’s rights in hospital contexts, held at the institution, seemed to us to be a potent act of dislocation of art from its traditional places and of reaching another public. While at the same time, in a very complex way, this very dislocation also perhaps exhausts its own potency because it was “art” (as if this delimitation involved a freedom of denunciation, that at the same time, meant its silencing because it is “not reality”).
Nor will I have space to report on the residency project’s second stage, which I conducted with the curator and artist Luiz Sérgio de Oliveira and that featured the artists Cristina Salgado, Hélio Carvalho, Gabriela Mureb and Roberta Barros – and that continued to count, of course, with the very close and fundamental presence of Ana Teresa Derraik, always strong, delicate and ethical, always conscious and involved in the political dimension of her work as a physician and ready to assume the risks arising from her advocacy for women’s rights. In this last stage, we had the joy of having an artistic residency at the Hospital included in the “Art_Care” project, coordinated by Izabela Pucu and Jessica Gogan at the Hélio Oiticica Municipal Art Center and were able to count on several partners who work at the interface between art and health. Thanks to funding from the Municipality of Rio de Janeiro, this second stage of the residency gave rise to the exhibition Nos limites do corpo [At the Limits of the Body] held at the Hélio Oiticica Municipal Art Center from November 2016 to February 2017. 3
Before closing my discussion of this experience, I want to draw from it a personal question that has been going round and around my mind ever since, and for which I do not have a clear answer: how did my training and experience as a psychoanalyst relate to this work as a curator? Could it be said that the monitoring and delineation of the process included a “clinical” dimension? I believe so, to some extent, but I do not think that this occurred in the sense that I ended up occupying the position of one who leads group conversation processes, as a kind of “therapist.” I believe that if the residency project had any “clinical” effect, this was due to the fact that it was structured as a process around listening and discussing the (desiring) position of each one of its participants, in the given context of political forces.
Places of Delirium
In December 2014, Paulo Herkenhoff, then Cultural and Artistic Director of the Rio de Janeiro Art Museum (MAR), invited me to curate an exhibition that already had a title: Lugares da Loucura [Places of Madness]. The project was part of the institution’s curatorial thematic program area – Art and Society in Brazil – aiming to discuss fundamental societal issues. To raise the taboo of madness today and take on the debate in the company of art – which had, as we know, a fundamental role in Psychiatric Reform – seemed to me to be important and even urgent. A necessity gathering force today, with the crisis hitting mental health services hard and the ultraconservative tendency of the Congress, running the risk of revising even some of the basic achievements of the anti-asylum struggle in Brazil. However, I did not agree with the idea of taking “madness” as a theme, as this tends to force an acceptance of its reification as a pathology and to make us lose sight of its complex and multifaceted social construction.
I then remembered the notion of delirium as Freud conceived it, as a tentative cure, and proposed that the exhibition be renamed Lugares do delírio [Places of Delirium]. This conception was very important in my training and especially in my doctoral dissertation, defended shortly after the experience at Foyer de L’Équipe, which consisted of a study on the notion of “loss of reality” in Freud’s work. This study was, of course, based on the question of psychosis, but it ended up taking me to art, through the Freudian idea that we all lose ‘reality’ and that it is not to accept it or to reject it pathologically, but rather to transform it, to some extent – as the artist does in his/her works. In this sense, psychotic delirium would be capable of denouncing the “paucity of reality” (“peu de realité” in the expression of the poet and artist André Breton) in which everyone lives, and show our power to transform it.4 Replacing “madness” with “delirium” meant, in this line of thought, a theoretical gesture of affirming the field of psychosis as a transformative power and of refusing its pathological delimitation characterized in terms of deficit. I hoped that such a gesture would make a claim for a political reach – and I now realize that it may have been intrinsically clinical, in the sense of reworking the question of “care” that I am trying to outline here. It undoubtedly took on the [kind of clinical] bet that I had experienced at Foyer de L’Équipe, employing such a posture as a key apparatus for reflection and curatorship.
Expanding the perspective of this project beyond mental health, it seemed to me important to also point out that the field of artistic production can be taken as a rigorous cultural arena for the construction of reality in a political dimension. We can say that in art, one has deliriums – that is, thoughts that shift from the usual tracks, the imaginary axes that fix the “common” reality from which we are alienated. Art rehearses models of the world and invites us to upturn prevailing imaginaries, putting ourselves outside ourselves – in the multiple places in which each one of us meets the other and finds himself or herself as another.
The term delirium thus seemed to me to name a kind of intersection between art and psychosis, and serve as a motor to rethink the historically rich relations between these fields, avoiding the idealization of the madman as an “artist” and the commonplace notion that approximates the artist with “the madman.” In addition, the term “delirium” takes on a very interesting sense of excess, pleasure and transgression in everyday parlance, in a radical summoning of the body of each one of us and of the game that establishes itself with other bodies in cultural places of delirium such as carnival, for example.
In this plural cross-over between art and madness in the cultural field and in this attempt to refuse categorizations and labels and blur boundaries and multiply directions, we try to affirm the diversity of the place and uniqueness of each subject. Such a “clinical” approach, drawing on a theoretical outline, as I have already pointed out, rather proposes a “constructive” and positive view on what would commonly be considered as a pathology and one of deficit. It was also fundamentally based on the choice of works that mixed artists identified with the psychiatric universe, such as Arthur Bispo do Rosário, Fernando Diniz and Raphael Domingues, and art world names such as Cildo Meireles, Anna Maria Maiolino and Laura Lima, stressing in all of them the power of reflection and transformation of reality. The curatorial project also mixed internationally recognized artists with those who were not well known and those from both inside and outside mental health networks. This diverse context included a series of works carried out in institutional settings – permanent workshops that take place on the border between art and treatment. For example, highlighting in particular the Poetic Psychiatry of Lula Wanderley and his collaborators at Espaço Aberto ao Tempo [Space Open to Time (EAT)] – and projects carried out by artists in partnership with mental health networks, such as artistic residencies, films and interviews (especially a program of artistic residencies at Ateliê Gaia – the artist/patient workshop/studio – housed at Bispo do Rosário Contemporary Art Museum.5
In this proposal, once again, we rejected the idea of “caring” for a certain segment of the population – people who experience intense psychic suffering – and to simply value the works of those artists that may be part of such segments. Instead, we attempted to adopt an ethical and political stance that would refuse such categorization and attempt to establish a platform for the dislocation of established borders and delimitations. We bet on the friction, the side-by-sideness between works by artists that would hardly ever be put together in current artistic discourse – for example, Cildo Meireles and Arthur Bispo do Rosário , as a generator of new vectors of reception for such works and of new questions for art and for life, including in the excess of life that manifests itself as the singularity of the subject, in so-called “madness”.
1. Cildo Meireles. Razão/Loucura (Reason / Madness), 1976/2017. Photo: Museu de arte do Rio de Janeiro (MAR).
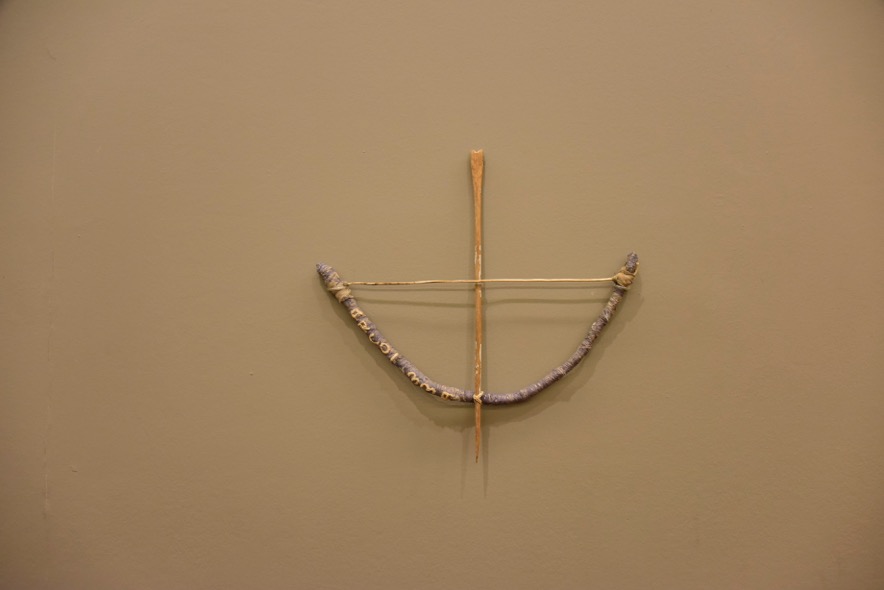
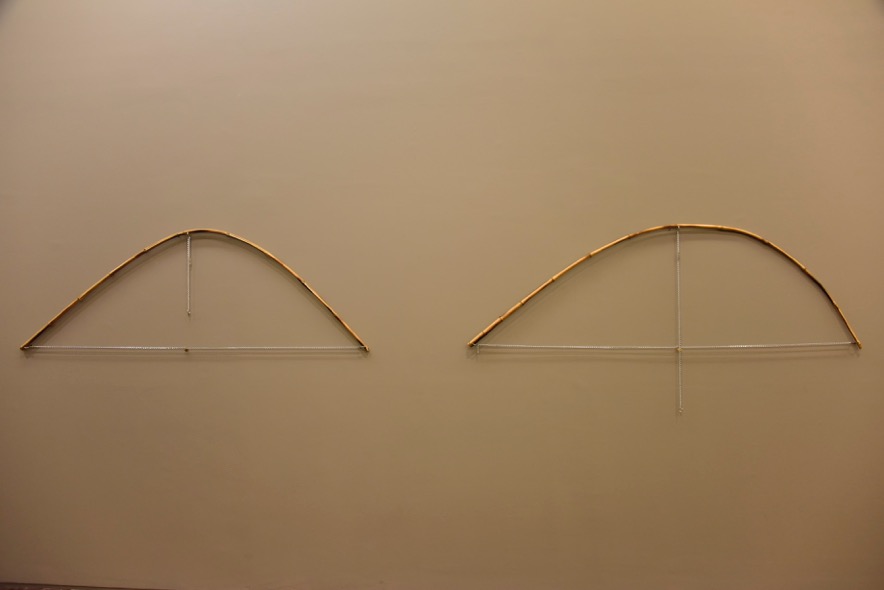
2. Installation view: Arthur Bispo do Rosário. Arco e Flecha “ORFA”, n/d. Museu Bispo do Rósario Arte Contemporânea. Photo: Museu de arte do Rio de Janeiro (MAR).

3. Installation view Cildo Meireles and Arthur Bispo do Rosário, Lugares do delírio, February 7th – September 17th, 2017, Museu de arte do Rio de Janeiro (MAR). Photo: Museu de arte do Rio de Janeiro.
The exhibition design and layout of the works in the museum space also tried to be faithful to this proposal. We rejected the false walls usually used as support for artworks, isolating them from the world, in favor of a contamination between various works. The need to think “spatially” led me to realize that the wall – like paper, in the case of writing or drawing – reveals an important structural element of reality, insofar as it is affirmed as a neutral surface capable of supporting representation of every thing in its ambit. Perhaps the quality of delirium – I was led to think – is the refusal of such support (which would correspond to the incidence of the very structure of the Symbolic, in Lacanian terms) in favor of the contamination of the elements of the world.
Along this contaminating line, the concept behind the first exhibition gallery was the refusal of the false wall, preferring horizontal planes of different heights, using tables instead of pedestals, in which the works were generally placed in groups. Scattered spatially, the tables prevented the establishment of predetermined or clear routes for visiting the exhibition, causing each spectator to navigate between them, tracing their own way. My hope was that at each point of this singular path, his/her gaze would mix together works and dislocate them, contagiously transforming them. This proposal echoed something important in the work of Arthur Bispo do Rosário: that fact that,interned for much of his life, in his studio-cells, the artist’s works were in a constant process of transformation and dislocation, relating to one another in a complex dance that questions the idea of a “work” that is unique and immutable.

Fig 4. View of the first room. On the left, on the wall, Fernando Diniz, Tapete digital [Digital Carpet]. By its side, Luis Carlos Marques Sem titulo [Untitled]. In the background, against the window, Bernardo Damasceno O M.A.R. vai virar Sertão [The Sea will Become the Desert (Sertão]. All other works are by Arthur Bispo do Rosário.>
In the second gallery, we refused the format that goes hand-in-hand with the use of the neutral vertical surface – the pedestal – to create the grid, a mesh of representation. Here there were no horizontal surfaces used to display works.
They were either hung from the ceiling (including video monitors) or attached to existing walls (only one wall surface was added in order to create the dark room needed for the projection of some audiovisual works). As part of this wall built for the exhibition, a huge leaning mirror (part of Laura Lima’s work Novos costumes [New Clothes] “broke” the verticality, “making the floor of the gallery take off,” in the words of the artist.

Fig 5. View of the second room. At the center, the mirror and support bars for the pieces of Laura Lima’s Novos costumes. On the left, on the wall, Wlademir Dias Pino O homem vegetal [The Vegetable Man]. In the background the group of works of Poetic Psychiatry by Lula Wanderley and collaborators.>
It may be unnecessary to point out that, in this project, the term “delirium” – naming the possibility of deviant paths, dislocations in relation to pre-established patterns – consists of a kind of performative or methodological notion that carries within itself a potential of political subversion. It is a radical defense of singularity, against all authoritarian and universalizing standardization. In the title “Places of Delirium”, this dimension is further reinforced by the affirmation of an indefinite plurality of “places” in which the delirious potential might be found. What is the place of delirium? The psychiatric hospital? The museum? Art? The world?
My proposal for a clinical position in curatorship and reflection in the field of the arts may simply be the defense of a delirious action, in an attempt to set reality itself into a transformative movement.
***
Tania Rivera
Tania Rivera is an essayist, psychoanalyst and professor in the art department and Postgraduate Studies in Contemporary Arts at the Federal Fluminense University (UFF). Highlights of her curatorial work include: Lugares do delírio (Museu de Arte do Rio (MAR), 2017 and the partnership with Luiz Sérgio de Oliveira in Nos limites do corpo (Centro Municipal de Arte Hélio Oiticica, 2016). She is author of the books Hélio Oiticica e a Arquitetura do Sujeito (2012, UFF) and O Avesso do Imaginário. Arte Contemporânea e Psicanálisce (2013, CosacNaify) among others.
____
1 For a classic text on psychoanalysis and definition of transference see Jean Laplanche and Jean-Bertrand Pontalis, The Language of Psycho-analysis (London: Karnac Books, 1988) [First published in 1973]
2 For those who might be interested in learning more about the institution and its theoretical basis I recommend the book by Alfredo Zenoni, L’Autre Pratique Clinique. Psychanalyse et Institution Thérapeutique. (Toulouse: Érès, 2009).
3 See the exhibition catalogue. Tania Rivera and Luiz Sérgio Oliveira, Nos limites do corpo (Rio de Janeiro: Centro Municipal de arte Hélio Oiticica, 2017). [Editor’s Note. E.N] For more information on the exhibition Nos limites do corpo also see part 4 of the vídeo Care as Method in this issue. [http://institutomesa.org/revistamesa/edicoes/5/portfolio/cuidado-como-metodo-en/?lang=en}
4 [Translator’s Note T.N.] In various publications André Breton’s term “peu de réalité” has been translated as “paucity of reality”. It was first introduced in his 1924 “Introduction au discours sur le peu de realité (Introduction to the Discourse on the Paucity of Reality). See translation: https://andrebreton.org/plaucityofreality.html [Accessed July 2018]
5 [E.N] See the case study on Bispo Rosário Contemporary Art Museum and especially the essay by Livia Flores on her artist residency as part of Lugares do delírio [http://institutomesa.org/revistamesa/edicoes/5/portfolio/livia-flores-carro-coracao-uma-videoexperiencia-en/?lang=en] and part 2 of the video Care as Method in this issue: [http://institutomesa.org/revistamesa/edicoes/5/portfolio/cuidado-como-metodo-en/?lang=en]
